1993
FMS Dental founded
The clinic that would become FMS International Dental Center began operations in Hyderabad.

All-on-4 is still a young protocol globally. FMS Dental, renowned as best dental implant clinic in India, has practised it for more than eighteen years — built on a far longer foundation in implant dentistry
The clinic that would become FMS International Dental Center began operations in Hyderabad.
The start of an implantology practice that now spans nearly three decades of continuous case experience.
Enabling implant placement in upper-jaw cases where bone height alone would have ruled it out.
Among the earliest centres in India to adopt the protocol following its international clinical validation.
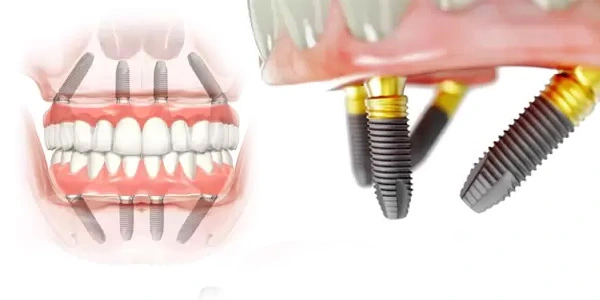
One of the only centre in India at that time to introduce Zygomatic implant protocol in combination with All-on-4.
All-on-4 surgery remains centralised at the Jubilee Hills flagship for surgical consistency.
FMS Dental didn't invent All-on-4 — the protocol originated with the Maló Clinic and Nobel Biocare internationally. It means FMS Dental was among the first clinics in Hyderabad India to bring it into routine practice in 2008, refined through close to two decades of continuous cases since.
Immediate-loading decisions — the insertion-torque judgment calls made mid-surgery — benefit directly from volume and repetition. A surgeon who has made that call thousands of times brings a different level of pattern recognition than one on their first hundred cases. Natural looking Prosthodontic options from senior Prosthodontists & top cosmetic dentists with an in-house lab and master technicians.
All-on-4 isn't "All-on-6 minus two." It's a different geometric solution — and the tilt is the entire point, not a compromise.
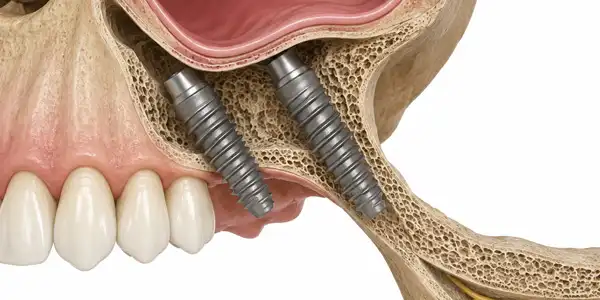
All-on-4 traces back to the Maló Clinic protocol, developed in the late 1990s and refined from earlier Branemark immediate-function research. Bone directly above the maxillary sinus or in front of the mandibular nerve canal is often too thin for a straight implant. Tilting the two posterior implants 30 to 45 degrees reaches that area of the bone and also without surgically altering the sinus or risking the nerve.
Before All-on-4, a patient with this kind of bone loss had essentially two options: a bone graft and a long wait, or a denture. Neither was a true fix. The graft added months — sometimes close to a year — before implants could even be placed, and grafted bone doesn't always integrate as predictably as the patient's own. A denture solved nothing structurally; it simply sat on top of a jaw that kept shrinking underneath it year after year. All-on-4 exists because someone asked a more precise engineering question: instead of building bone where there isn't any, can the implant simply be angled towards the bone that's already there? Worked out through cadaver and clinical studies in the late 1990s, the answer was yes — provided the angle, the spacing between implants, and the rigidity of the cross-arch connection were all engineered correctly together. Get any one of those three wrong and the structure fails under normal biting force within a few years. Get all three right, and it can carry full function from the very first day.
Tilting the posterior implant keeps it anterior to the sinus wall, or forward of the mental nerve's exit point — frequently avoiding a sinus lift or nerve repositioning entirely.
The unsupported bridge length behind the last implant is where bending force concentrates. The tilt shortens this arm, reducing leverage on the rear implants.
A tilted implant engages more linear bone than the same implant placed vertically — useful where vertical bone height is limited.
A restored arch is only as good as the prosthetic it carries; Dr. Kavya and Dr. P. Parthasaradhi Reddy design and fit every final prosthesis to function precisely and look natural from day one, for perfect replacement.
Maximised "anteroposterior spread" reduces rocking forces on the bridge — what makes immediate loading viable at all.
A longer vertical implant sounds like the simpler fix, but it has nowhere to go once it reaches the sinus floor or the nerve canal — length can't solve an anatomical wall. Tilting moves around the obstacle instead of pushing towards it, which is the actual engineering insight behind the whole protocol.
Below roughly 30°, the implant doesn't clear the sinus or nerve with reliable safety margin. Beyond about 45°, the angle starts working against the implant — bite force is transmitted less efficiently along its length, and the prosthetic connection becomes harder to seat accurately. That range is the engineering balance point between the two failure modes.

Because the posterior implants reach bone that's still there — not bone already resorbed — most patients with moderate bone loss don't need a graft before surgery.
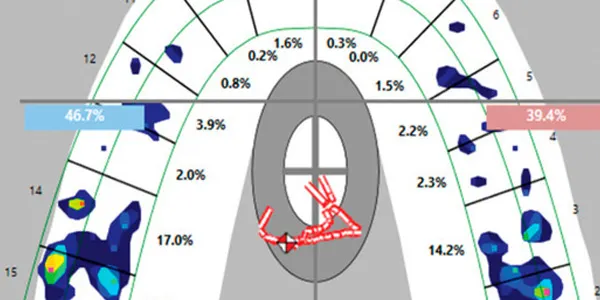
Bone-specific, not just tooth-loss-specific. The answer depends on what a CBCT scan shows at four exact points.
The question patients usually ask first is "am I too old," or "is my bone too far gone." Neither is actually the deciding factor. All-on-4 candidacy comes down to a much narrower, more specific question: at the four exact points a digital plan would use — two near the front of the jaw, two further back at the planned tilt angle — is there enough bone, of sufficient density, to grip a titanium implant firmly enough for it to carry load immediately? Everything else, age included, is a secondary consideration that gets weighed once that core question is answered.

Once several teeth in an arch are compromised, treating each individually with its own implant becomes more invasive, more expensive, and structurally weaker than restoring the whole arch as one connected system.

Specifically: enough vertical height at the two front sockets, and enough density just anterior to the sinus or nerve canal to seat the tilted pair at the planned 30–45° angle without compromise.

Controlled diabetes (not necessarily diabetes-free), no active periodontal infection at the surgical site, and cardiovascular status cleared for a procedure that can run four to five hours.
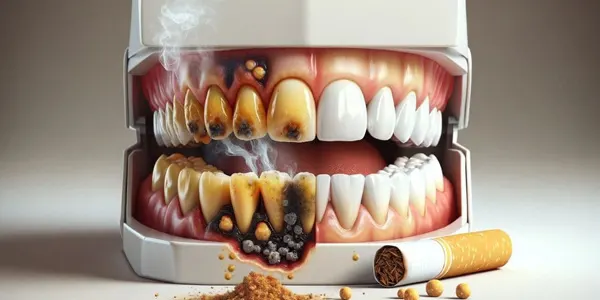
Nicotine constricts the small blood vessels that supply healing bone. The biggest risk window is the first 8–10 weeks after surgery — exactly when smoking does the most damage to integration.
If even the angled posterior position lacks sufficient bone, four implants can't achieve reliable primary stability — this is the specific point where zygomatic implants, anchored in the cheekbone rather than the jaw, become the relevant alternative.
Documented heavy bruxism on borderline bone concentrates more force per implant than four can comfortably carry long-term — this is precisely the scenario All-on-4 Plus exists to address, covered just below.

Both directly impair the bone's ability to heal around titanium. Treatment is sequenced rather than declined outright — stabilise the underlying condition first, then reassess candidacy with a fresh CBCT.

Implants don't move with growing bone the way natural teeth do. Placed before skeletal maturity, an implant can end up in the wrong position — too far forward, too far back, or at the wrong height — as the jaw continues to develop around it.
A CBCT scan at your assessment maps bone height, width, and density at all four planned positions before any recommendation is made — the same scan that rules All-on-4 in also rules it towards a different protocol when that's the honest answer.
When one or two more implants are the right call — and exactly when they aren't.
All-on-4 Plus is the same tilted-implant geometry and same-day loading philosophy as standard
All-on-4, with one or two additional implants at intermediate points along the arch — for cases where four alone would carry more load, long-term, than is biomechanically comfortable.
Adding one or two implants doesn't change the underlying logic of the protocol; it changes the math. Four implants spread a given bite force across four contact points. Six spread the same force across six — each implant individually carries less, which matters over a 15 or 20-year horizon in patients who put unusually high load through their bite, or whose arch is simply wider than average and would otherwise leave a longer unsupported span between implants.
This is a CBCT-driven decision, not a preference-driven one. Dr. Shailaja Reddy recommends All-on-4 Plus specifically when imaging shows a broader-than-average arch, a documented history of heavy bruxism or high bite force, or bone density and volume that comfortably support six well-distributed implant sites rather than four under more concentrated load. If a case doesn't show any of these factors, standard All-on-4 already does the job completely — the additional surgical time, the one or two extra implants, and the higher cost aren't recommended without a specific clinical reason behind them. It is never offered as a default upgrade.
Implants
Average arch, average bite force.

Implants
Wider arch or high bite force.
Comparing against All-on-6, zygomatic, or conventional full-arch instead? See our full mouth implant options page.
Both materials sit on the same four implants. The difference is what you'll notice day to day, and what it takes to keep looking right ten years from now.

A milled titanium bar provides the rigid internal framework; denture-grade acrylic resin is layered over it to form the visible teeth and gum-coloured base. This is also the standard material used for the provisional bridge fitted on surgery day itself, so many patients are already familiar with how it feels before the definitive version is even made.
It's noticeably lighter than zirconia, which some patients prefer for comfort, and if a tooth chips or a clip needs adjusting, it can usually be repaired chairside the same day rather than sent out to a lab. The trade-off is that the acrylic surface wears and can pick up staining over many years of normal use — manageable, but worth knowing upfront.

A single solid block of zirconia is milled to form both the structural framework and the visible teeth in one continuous piece — there's no separate acrylic layer that can wear down, discolour, or delaminate over time. It's also the material most resistant to the kind of surface staining that comes from years of tea, coffee, or turmeric-heavy food.
The trade-off runs the other way from acrylic: zirconia is heavier in the hand, and because it's milled as one solid piece, a chip or fracture can't be patched chairside — it requires a new piece to be milled in the lab. For patients who specifically don't want to think about the bridge again after it's fitted, this is usually still the preferred choice despite that.
ALL-ON-4 — is a multi-specialist procedure. This is Our Expert Implant Dentists team.







All-on-4 dental implant cases involve anatomy that extends beyond implant placement — sinus cavities, cranial base structures and complex occlusal loading. FMS having Oral & Maxillofacial Surgeons, Prosthodontists and experienced implantologists plan together for delivering better end results. At FMS Dental, complex surgical decisions are reviewed jointly before the patient enters the operating room.






