
Pterygoid dental implants offer a permanent fixed teeth solution for patients with severe upper jaw bone loss, no bone grafts, no sinus surgery, no lengthy waiting periods. The implants anchor into the dense bone behind the upper jaw that remains intact even after years of tooth loss, making this procedure possible for patients who have been turned away elsewhere. Fixed teeth are placed within 24-72 hours of surgery and the 10-year success rate stands at 94-98%.
The entire treatment, from 3D scan to final prosthesis, is completed in a single surgical visit with 4–6 implants per jaw. FMS Dental, Hyderabad has been performing this procedure at its NABH - accredited facility in Hyderabad with over 25,000 implants placed across all centres. Treatment starts from ₹4,50,000, with Nobel Biocare and Straumann implant options available.
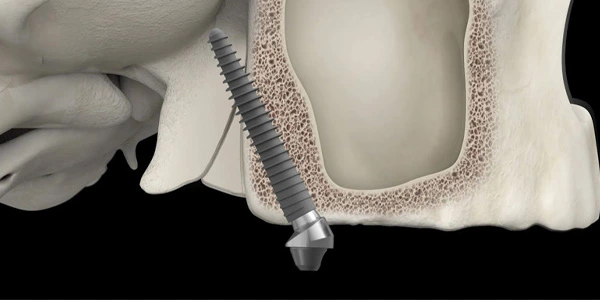
Pterygoid implants are long-angled titanium implants (18–25 mm) placed at 45–55° into the pterygoid process — the dense cortical bone formed by the sphenoid and palatine bones immediately behind the upper jaw — to anchor a complete fixed upper-arch dental prosthesis. The technique eliminates the need for bone grafting or sinus augmentation, making it the primary solution for patients with severe maxillary (upper jaw) bone loss. It was pioneered by Jean-François Tulasne in 1989 and has a documented 10-year survival rate of 94–98%.
This guide covers the anatomy, history, surgical protocol, candidacy criteria, published clinical evidence, recovery, and cost. It is written for patients researching this treatment and for clinicians seeking a reliable reference. Every factual claim is grounded in peer-reviewed literature or clinical measurement data.
This page covers Pterygoid — the upper jaw full-arch pterygoid implant protocol specifically. For lower jaw implants, full-mouth (upper + lower) rehabilitation, or zygomatic implants, see the respective dedicated pages at FMS Dental.
1989 by Jean-François Tulasne, published IJOMI 1992
18–25 mm, placed at 45–55° angulation
Pterygoid process (sphenoid + palatine bone)
≥35 Ncm insertion torque for immediate loading
94-98% (Rodríguez et al. systematic review, 2020)
No bone graft required. No sinus lift required.
Within 24-72 hours of surgery
2 pterygoid + 2-4 anterior implants = 4-6 total
₹4,50,000 - ₹6,00,000+ (brand and prosthesis dependent)
What pterygoid implants are, where they anchor and why that anatomical zone works even when the jaw has severely atrophied.
When teeth are lost, the alveolar bone — the ridge of jawbone that held the tooth roots — begins to resorb. Over years of tooth loss, denture wear, or periodontal disease, this resorption can be severe. In the posterior upper jaw, two additional factors accelerate the problem: the maxillary sinus expands downward (pneumatisation) as surrounding bone disappears, and the upper jaw naturally loses vertical height faster than the lower.
Standard dental implants require a minimum alveolar bone height — typically 10 mm. When the alveolar ridge has resorbed and the sinus has expanded, that space no longer exists. The traditional answer was to rebuild it: either graft bone into the sinus (sinus lift) or augment the ridge with harvested bone — procedures adding 6–12 months to treatment and carrying their own failure rates.
The pterygoid process of the sphenoid bone is anatomically distinct from the alveolar ridge. It forms part of the skull base and does not resorb when teeth are lost. It is always present. And crucially, it is dense cortical bone — the same type of bone that provides the best implant anchorage. A pterygoid implant bypasses the lost alveolar bone entirely, anchoring in this cortical structure.
An ideally placed pterygoid implant engages bone in three anatomical zones, each contributing to overall stability:
This multi-zone cortical engagement is why pterygoid implants achieve the high insertion torques (35–55 Ncm) required for immediate loading. The density of the pterygoid process means this is not dependent on alveolar bone quality at all.
The pterygoid implant trajectory passes posterior to the maxillary sinus — not through it. No sinus membrane is elevated, perforated, or augmented. This eliminates one of the most common sources of complication in posterior upper jaw implant surgery.
The success of a pterygoid implant depends on engaging multiple anatomical structures that provide exceptional cortical bone support. Each anatomical zone contributes to the overall stability of the implant and allows immediate loading without the need for bone grafting or sinus augmentation.
Primary anchor. Dense cortical bone at the skull base. Present regardless of alveolar ridge resorption. Implant tip engages here for maximum stability. Minimum 10-12 mm bone depth confirmed by CBCT pre-surgically.
Intermediate zone traversed by the implant body. Contributes additional cortical bone contact. Combined with pterygoid bone engagement, enables bicortical or tricortical anchorage.
Entry point for the implant. Bone density here is variable — the implant must pass through this zone into the denser palatine and pterygoid bone beyond. CBCT confirms adequacy.
Posterior and superior angulation maximises bone contact length across all three zones. Angulated multi-unit abutments (17–30°) compensate for the angle at the prosthetic interface.
The surgical trajectory passes entirely posterior to the sinus. No sinus wall elevation, no perforation risk, no healing period for sinus augmentation required.
The pterygopalatine fossa and descending palatine artery lie medial to the pterygoid implant trajectory. 3D CBCT planning and surgical guides maintain safe margins. Neurovascular injury risk is low in experienced hands.
Pterygoid implants were introduced by French oral and maxillofacial surgeon Jean-François Tulasne in 1989. His landmark publication in the International Journal of Oral and Maxillofacial Implants (1992) documented the first systematic clinical use of pterygoid implants for severely atrophied upper jaws, establishing both the anatomical rationale and the surgical protocol that remains in use today.
Tulasne's clinical reasoning was precise: the pterygoid bone had been entirely overlooked as an implant anchor zone, yet it offered everything required for successful osseointegration - high cortical density, reliable anatomy, consistent depth (≥14 mm in anatomical studies) and complete separation from the maxillary sinus. By contrast, the prevailing approach, bone grafting and sinus augmentation, added 6-12 months of treatment, carried graft failure rates of 10-20% and required the patient to undergo two to three surgeries instead of one.
Osseointegration — the direct structural and functional connection between living bone and a titanium implant surface — was established by Per-Ingvar Brånemark in the 1960s. The quality of osseointegration is directly related to the quality of bone contact at implant placement. Cortical bone, being denser than cancellous (trabecular) bone, provides superior primary stability, resists micro-motion during early healing, and integrates with fewer vascular channels - meaning the titanium oxide surface on modern implants plays a more dominant role.
The pterygoid process is predominantly cortical. When a pterygoid implant achieves bicortical engagement, anchoring in both the palatine bone and the pterygoid process, it achieves insertion torques of 35-55 Ncm. This is above the threshold required for immediate loading, which is why the Pterygoid protocol can deliver fixed provisional teeth within 24-72 hours of surgery.
Early pterygoid implants (1989-2000) used machined titanium surfaces with relatively slow osseointegration. Modern implants use sandblasted and acid-etched (SLA) or anodised surfaces with micro and nano-scale topography, reducing osseointegration time from 6 months to 6-8 weeks in cortical bone. This is why modern pterygoid implants can be loaded earlier and achieve higher long-term success rates than early cases would suggest.
The term Pterygoid refers specifically to the full upper-arch rehabilitation protocol using pterygoid implants as the posterior anchors. It distinguishes this full-arch concept from single pterygoid implants placed to restore individual missing teeth in the posterior maxilla.
Tulasne JF (1992). Osseointegrated fixtures in the pterygoid region. In Worthington P & Brånemark PI (eds.), Advanced Osseointegration Surgery. Quintessence, Chicago.
The specific implant configuration, prosthetic system, and planning requirements for full upper-arch rehabilitation.
A complete Pterygoid upper arch uses 4 to 6 implants total:
This configuration replicates the natural load distribution of a full upper dentition. The pterygoid implants bear molar and premolar forces; the anterior implants bear incisor forces. Together they support a full fixed arch without any posterior alveolar bone.
In cases of extreme total upper jaw atrophy where even the front alveolar bone is insufficient for anterior implants, 4 bilateral pterygoid implants can support the full arch without anterior fixation. This is a more advanced protocol requiring specialist CBCT planning and a highly experienced implantologists and maxillofacial surgeons' team. It is reserved for the most severe cases.
Because pterygoid implants exit the posterior palate at steep angles, angulated multi-unit abutments (typically 17° or 30°) are used to create a parallel prosthetic platform despite the angular implant placement. This allows standard laboratory prosthetic workflows on a flat-plane framework.
The prosthetic sequence is: immediate acrylic provisional (day 1-3) → osseointegration (months 1-4) → final prosthesis (month 4-6). Final prostheses are typically full-arch zirconia-on-titanium frameworks or monolithic zirconia bridges, chosen for strength, aesthetics and longevity.
Pterygoid implant placement requires Cone Beam Computed Tomography (CBCT) before surgery. The pterygoid bone lies adjacent to the pterygopalatine fossa, the descending palatine vessels, and the medial pterygoid muscle. These structures require precise mapping. CBCT provides:
Exact measurement of pterygoid bone depth (minimum 10-12 mm required)
3D visualization of implant trajectory and safe angulation
Identification of any anatomical variants or pathology
Data for surgical guide fabrication (where used)
No experienced pterygoid implantologist plans or places these implants without 3D CBCT imaging. A 2D panoramic X-ray cannot provide the anatomical information required for safe pterygoid implant placement. If you are being offered pterygoid implants without a CBCT scan, seek a second opinion.
For comprehensive Pterygoid cases, a 3D-printed surgical guide is fabricated from the CBCT data. The guide constrains the drill trajectory to within 0.5-1.0 mm of the planned position, reducing placement error and improving predictability, particularly important given the steep angulation and proximity to adjacent structures in pterygoid surgery.
Who qualifies for Pterygoid and what conditions make it unsuitable or inadvisable.
Many patients told "you cannot have implants due to bone loss" have not been evaluated specifically for pterygoid implant candidacy. The pterygoid bone is a separate anatomical structure from the alveolar ridge, and its suitability requires CBCT assessment — not a clinical inspection alone. A CBCT evaluation at FMS Dental determines candidacy definitively.
What happens from the day of evaluation to the placement of your permanent prosthesis.
Cone Beam CT imaging maps your jaw anatomy in three dimensions. Pterygoid bone depth, implant trajectory, sinus position, and adjacent structures are assessed. Digital smile design is completed. A surgical guide may be fabricated for precision placement.
Haematological workup confirms systemic health. Active gum disease or infection is treated. The acrylic provisional full-arch prosthesis is fabricated in advance — so it can be fitted within hours of surgery rather than after a lab delay.
Day-case procedure under local anaesthesia (IV sedation optional). Pterygoid implants are placed bilaterally at 45–55° through the tuberosity into the pterygoid process. Anterior implants are placed simultaneously. Total procedure: 2-4 hours. Patient returns home same day.
Insertion torque is verified intraoperatively. When stability is confirmed (≥35 Ncm), angulated abutments are connected and the provisional fixed arch is attached. Patients leave with fixed teeth... no removable denture, within 24–72 hours.
At the 3-month review, integration is confirmed by resonance frequency analysis and periapical radiographs. The final zirconia-on-titanium or monolithic zirconia full-arch prosthesis is fabricated and fitted. Diet restrictions are fully lifted.
Immediate loading — placing fixed teeth the same day as surgery — is not assumed. It is a clinical decision made during surgery based on measured implant stability. Insertion torque is recorded for each pterygoid implant using a calibrated torque wrench. When torque reaches ≥35 Ncm, immediate loading proceeds. When torque is marginal (25-35 Ncm), the surgeon may elect early loading at 6–8 weeks. When torque is insufficient (<25 Ncm), conventional loading at 3-4 months is indicated.
Resonance Frequency Analysis (RFA) using a Penguin or Osstell device provides a secondary stability measurement expressed as an ISQ value. An ISQ ≥70 correlates with adequate primary stability for immediate loading in cortical bone.
The most consistent feedback from FMS Dental's pterygoid patients: the experience is significantly more manageable than anticipated. Local anaesthesia is highly effective in the pterygoid region. Patients feel pressure and vibration during surgery — not pain. Post-operative swelling peaks at 48 hours and is well-managed with standard anti-inflammatories. Most patients return to desk work within 3-5 days.
Anaesthesia options at FMS Dental: Local anaesthesia (standard), or general anaesthesia (for complex bilateral cases with additional procedures). All are available at FMS Dental's NABH - accredited surgical facility.
Peer-reviewed studies, systematic reviews, and the long-term data that supports Pterygoid as an evidence-based standard of care.
Documented the original surgical protocol and clinical rationale for pterygoid implant placement. Established that the pterygoid process provides reliable, high-stability anchorage independent of alveolar ridge condition. Formed the anatomical and biomechanical basis for all subsequent work.
60 patients with severely atrophied posterior maxilla. Cumulative 5-year survival rate: 95.3%. No implant losses after Year 1 of loading. Concluded pterygoid implants are a predictable, graft-free alternative for severe posterior bone loss, with outcomes equivalent to standard implants in healthy bone.
CBCT and cadaveric dissection across 50 specimens. Found consistent pterygoid bone depth ≥14 mm across all specimens. Confirmed that correct implant angulation maintains safe margins from the pterygopalatine fossa and descending palatine artery. Established anatomical safety benchmarks still used for surgical planning.
18 studies, 412 patients, 661 implants. Weighted mean 10-year survival: 97.1%. No statistically significant difference from standard implants in healthy bone. Mean patient satisfaction: 9.1/10. Identified smoking, poor bone quality, and surgical inexperience as primary risk factors. Concluded pterygoid implants are an evidence-based treatment for maxillary atrophy.
Evidence summary: Three decades of peer-reviewed data across hundreds of patients and multiple systematic reviews consistently confirms Pterygoid delivers 10-year survival rates of 94-98% — indistinguishable from standard implants in healthy bone. This is not an experimental technique. It is a mature, evidence-based protocol for a specific clinical indication.
References: Tulasne JF (1992) Int J Oral Maxillofac Implants 7(1):81–94 · Balaji SM (2002) J Oral Maxillofac Surg 31(2):98–109 · Graves SL (2014) J Oral Implantol 40(4):452–462 · Rodríguez X et al (2020) Int J Oral Maxillofac Implants 35(3):e61–e75
Year FMS started pterygoid implants
Years implant clinical experience
Implants placed across all centres
Rating across 4,487+ reviews
Accredited hospital — highest quality standard
Transparent pricing across every implant tier at FMS Dental, Hyderabad.
Pterygoid implants are long titanium implants (18–25 mm) placed at 45–55° into the pterygoid process — the dense cortical bone formed by the sphenoid and palatine bones behind the upper jaw — combined with anterior implants to support a complete fixed upper-arch dental prosthesis. The technique eliminates bone grafting and sinus surgery. It was pioneered by Jean-François Tulasne in 1989 and has a 10-year survival rate of 94–98%.
Pterygoid dental implants were invented by French oral and maxillofacial surgeon Jean-François Tulasne in 1989. His clinical findings were published in the International Journal of Oral and Maxillofacial Implants in 1992, establishing the anatomical rationale and surgical protocol that forms the basis of all current pterygoid implant techniques.
The 10-year survival rate for Pterygoid implants is 94–98%, based on multiple peer-reviewed studies. A 2020 systematic review by Rodríguez et al. covering 18 studies and 661 implants reported a weighted mean survival of 97.1% — statistically comparable to standard implants placed in healthy bone.
At FMS Dental, Hyderabad, Pterygoid treatment starts from ₹1,10,000 for Alpha Bio Tec budget implants and reaches ₹2,20,000+ for Nobel Biocare or Straumann premium full-arch solutions. Cost depends on the number of implants, brand, and prosthetic material (acrylic vs zirconia). All prices include the CBCT scan, surgery, provisional prosthesis, and final restoration.
No. Pterygoid is specifically designed to eliminate bone grafting. The pterygoid implants anchor in the pterygoid process — bone that is consistently present and does not resorb with tooth loss — bypassing the deteriorated alveolar ridge entirely. No bone graft, no sinus lift, no additional healing time.
In most cases, yes. When insertion torque is ≥35 Ncm (confirming adequate primary stability in the pterygoid bone), a fixed provisional full-arch prosthesis is loaded within 24–72 hours of surgery. This is called immediate loading. The final zirconia prosthesis is fitted after full osseointegration at 3–4 months. Immediate loading suitability is confirmed during surgery — not pre-assumed.
Pterygoid implants (18–25 mm) anchor in the pterygoid process behind the upper jaw and are used for posterior maxillary bone loss. Zygomatic implants (30–52 mm) anchor in the zygomatic (cheekbone) complex and are used for extreme total maxillary bone loss when pterygoid bone is also insufficient. Pterygoid implants are less invasive and the first-line choice. Zygomatic implants are reserved for the most severe cases where pterygoid anchorage is inadequate.
With proper oral hygiene and 6-monthly professional maintenance, pterygoid implants are designed to last a lifetime. Clinical data across 30+ years shows sustained high survival rates at 10 years (94–98%). Nobel Biocare and Straumann implants carry lifetime manufacturer warranties. The prosthetic bridge typically requires replacement every 10–15 years (zirconia) or 7–12 years (acrylic).
Risks include: early implant failure (2–6% in non-ideal candidates), peri-implantitis (preventable with proper hygiene), intraoperative bleeding, swelling, and prosthetic complications. Pterygoid-specific risks — proximity to the pterygopalatine fossa — are mitigated by 3D CBCT planning and surgical guide use. Serious complications are uncommon in experienced hands. The most significant risk factors are heavy smoking, uncontrolled diabetes, insufficient CBCT planning, and surgeon inexperience with the technique.
FMS Dental began placing pterygoid implants in 2015 — making it one of the first centres in South India to adopt the technique. With 30+ years of overall implant experience, 25,000+ implants placed, fellowship-trained implantologists, a NABH - accredited facility, in-house 3D imaging, and an in-house digital prosthetics lab, FMS Dental offers the depth of expertise and infrastructure that pterygoid implant surgery requires.
📍 Jubilee Hills, Hyderabad 📍 Kondapur, Hyderabad 📍 Secunderabad 🕘 Mon–Sat, 8:30 am – 9:30 pm